Moral Distress
The rapidly evolving pandemic has created unprecedented moral distress among health care workers asked to work under extreme circumstances. Moral distress refers to the unique stress that professionals may experience if they are unsure about, conflicted with, or not able to fulfill their ethical obligations. Shortages of personal protective equipment and rapidly changing infectious disease policies add to the stress healthcare workers experience while balancing concerns for their own personal health against their duty to care. Facing uncertainty around effective treatments, managing scarce resources, and personal exposure to mortality and suffering, they find themselves challenged to meet the needs of patients, families, and colleagues.
How is moral distress different than regular job stress?
While there are many sources of stress in healthcare, moral distress is specifically associated with the ethical dimensions of practice and concerns related to difficulty in navigating practice while upholding professional values, responsibilities and duties. Moral distress is the result of a perceived violation of one’s core values and duties, concurrent with a feeling of being constrained from taking ethically appropriate action.
It may be helpful to distinguish between moral distress and identifying ethical issues or questions. Although they may overlap – resources for addressing them may vary. In general, ethics committees and ethics consult services exist to help health care professionals to identify and address ethical questions like who should make these decisions and what decisions should be made. Moral distress resources could involve the same ethics committee/consult resources, but the attention is slightly different and shifts to how health care professionals can live out the ethical commitments that have been identified. If you don’t have access to an ethics resource, some of the resources mentioned on this website could be helpful.
The term “moral distress” was first defined by Andrew Jameton on 1984 as a phenomenon in which “one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action” (Jameton, 1984) The concept has evolved from the first and influential description by Jameton that referred only to nurses. Moral distress now refers to the experience of all health care professionals and not just under the conditions of constraint but also conflict or uncertainty. (Campbell SM, Ulrich CM, Grady C. A broader understanding of moral distress. American Journal of Bioethics. 2016;16(12):2-9.)
There is a high degree of variability in how moral distress manifests itself; however, it has been described consistently as creating debilitating frustration, anger, guilt, anxiety, withdrawal, and self-blame.
Moral Residue and Crescendo Effect
In his attempt to describe moral distress, Jameton identified two aspects of moral distress: initial distress, which happens at the onset of a crisis, and reactive distress, which has a lingering effect long after the crisis has passed (Jameton, 1993).6 In 2000, Webster and Bayliss referred to the lingering distress phenomenon as “moral residue” and defined it as “that which each of us carries with us from those times in our lives when in the face of moral distress we have seriously compromised ourselves or allowed ourselves to be compromised” (Webster, G., & Bayliss, F. (2000, p. 208).7 In 2009, Epstein and Hamric expanded on the moral residue definition, in light of the distinctions initially identified by Jameton, to include the term “Crescendo effect” defined as “the repeated exposure to situations that give rise to moral distress and results in repeated threats to moral integrity ” (Epstein and Hamric, 2009, p.340).8 Epstein and Hamric argued that the two features attributed to the “Crescendo effect” are:
1) The distress of a particular episode of moral distress is magnified the longer the episode lasts;
2) The resulting moral residue amplifies the distress of subsequent experiences of moral distress.
The combination of these two factors describe the crescendo effect over the course of time. Therefore, the level of residual moral distress increases with every exposure to a morally distressing occasion even after it is resolved (Corley, 1995; Hamric & Blackhall, 2007; Epstein 2008).
The importance of Peer Group in recognizing Moral Distress:
The ‘4 A’s’ Model
The following prominent model called ‘The 4A’s to Rise Above Moral Distress’ 3, was proposed by The American Association of Critical Care Nurses to help those who experience moral distress. The aim of this approach is to identify and reduce moral distress by responding through the following four steps (AACN, 2005; Rushton, 2006).
Ask: Help individuals to ask and identify whether the symptoms they are experiencing are associated with moral distress. The objective of this step is to enable the individual to become aware that moral distress is present, if it is indeed present.
Affirm: Following the identification step, the individual is encouraged to affirm his/her distress and proceed with the commitment of taking care of his/herself. This commitment involves validating the individual’s perceptions and feelings with others; while affirming their professional duty to act. The objective of this step is to enable the individual to make a commitment to address moral distress.
Assess: Once the commitment is made by the individual to address moral distress, they can begin to assess the sources of their experience and determine whether it is personal or environmental. The goal of this step is to encourage the individual and confirm that ‘you are ready to make an action plan’.
Act: This step prepares the individual to take the action set out in their action plan and to begin implementing strategies that result in the desired changes while also expecting some set-backs. The goal of this step is to help the individual preserve their authenticity and moral integrity.
Definitions
Moral Distress: The concept has evolved from the first and influential description by Andrew Jameton in 1984 where moral distress occurs when a nurse “knows the right thing to do,” (p.6) but institutional constraints make it nearly impossible to pursue the right course of action. . Moral distress now refers to the experience of all health care professionals and not just under the conditions of constraint but also conflict or uncertainty. (Campbell, Ulrich & Grady, 2016)
Moral Resilience: The capacity of an individual to sustain or restore their integrity in response to moral complexity, confusion, distress or setbacks. (Rushton, 2016) The use of moral resilience is an effort to move beyond the strictly negative features of moral distress/moral injury and concentrate on the positive aspects of addressing moral distress/injury and the ethical issues in practice.
Moral Injury: Conflicts with an individual’s values, beliefs, and moral outlook that can have long term mental health effects. The concept comes from the traumatic stress literature and started with events associated with the battlefield. In early descriptions, potentially morally injurious events are those that include “perpetrating, failing to prevent, bearing witness to, or learning about acts that transgress deeply held moral beliefs and expectations.” (Griffin BJ et al, 2019). To a large extent, the nursing literature uses the term ‘moral distress’ and the physician literature uses the term ‘moral injury.’
Moral Distress Rounds: Small group meetings facilitated by people trained in ethics where the morally distressing features of a situation are discussed. Participants describe their experiences, the ethically relevant features are described, and then discussion occurs about what can be done to mitigate moral distress at the bedside, at the unit level and at the institutional level. These small groups can be discipline specific or multidisciplinary. At the end of the meeting the discussion is summarized, and action items assigned. (Hamrick and Epstein, 2017)
Ethics Consultation: A service provided by people trained in ethics to help health care professionals, patients, and/or families identify and address ethical issues in patient care. Ethics consultants act as advisors and educators, not clinical decision makers. Ethics consults can be performed by an individual, a team or a full ethics committee. Ethics Consultation is one of the three major tasks of an ethics committee along with writing and revising policies that have ethical dimensions and providing ethics education. The Joint Commission requires hospitals to have a mechanism in place to help staff address ethical issues. Ethics Committees are also present in many home health care agencies, hospices and long-term care settings but to a lesser extent than in hospitals. (American Society for Bioethics and Humanities, 2011)
How is the COVID-19 pandemic adding to the risk of healthcare workers (HCWs) experiencing moral distress?
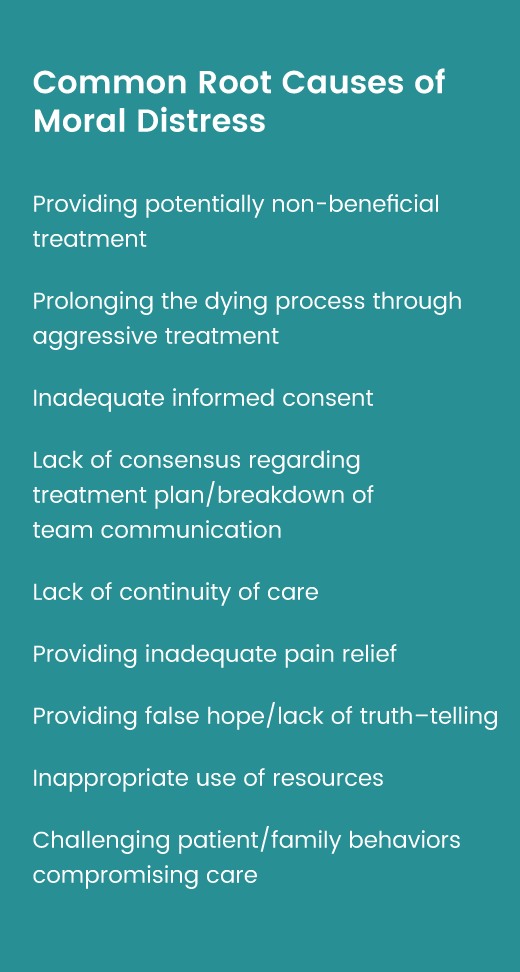
In addition to the common root causes of moral distress, the pandemic has added additional circumstances that put HCWs at risk of experiencing moral distress. These include:
Worries about “taking it home with you” and potentially transmitting the virus to loved ones or community members
Decisions about allocating limited resources or a lack of resources
Being put at personal risk by an unprepared healthcare system
Visitation restrictions for the critically ill and dying
The time it takes to put on PPE prior to a Code response, which leads to worse outcomes
Social justice concerns
Structural Racism
References:
(1) Jameton, A. (1984). Nursing practice: The ethical issues. Englewood Cliffs, NJ: Prentice-Hall.
(2) Hardingham, L. B. (2004). Integrity and moral residue: Nurses as participants in a moral community. Nursing Philosophy, 5(2), 127-134.
(3) http://www.emergingrnleader.com/wp-content/uploads/2012/06/4As_to_Rise_Above_Moral_Distress.pdf
(4) American Association of Critical Care Nurses (AACN). (2005). AACN standards for establishing and sustaining healthy work environments. Retrieved from https://www.aacn.org/nursing-excellence/standards/aacn-standards-for-establishing-and-sustaining-healthy-work-environments
(5) Rushton, C. H. (2006). Defining and addressing moral distress: Tools for critical care nursing leaders. AACN Advanced Critical Care, 17(2), 161-168.
(6) Jameton, A. (1993). Dilemmas of moral distress: Moral responsibility and nursing practice.AWHONNS Clinical Issues in Perinatal & Womens Health Nursing, 4(4), 542-551.
(7) Webster, G., & Bayliss, F. (2000). Moral residue. In S. Rubin, & L. Zoloth (Eds.), Margin of error: The ethics of mistakes in the practice of medicine. Hagerstown, MD: University Publishing Group, Inc.
(8) Epstein, E. G., & Hamric, A. B. (2009). Moral distress, moral residue, and the crescendo effect. Journal of Clinical Ethics, 20(4), 330-342.
(9) Corley, M. C. (1995). Moral distress of critical care nurses. American Journal of Critical Care, 4(4), 280-285.
(10) Hamric, A. B., & Blackhall, L. J. (2007). Nurse-physician perspectives on the care of dying patients in intensive care units: Collaboration, moral distress, and ethical climate. Critical Care Medicine, 35(2), 422-429.
(11) Epstein, E. G. (2008). End-of-life experiences of nurses and physicians in the newborn intensive care unit. Journal of Perinatology, 28, 771-778.